You've finally got a breakout under control. The spot has flattened, the tenderness has gone, and you're expecting your skin to move on. Instead, a stubborn brown, tan, or grey mark stays behind and seems to outlast the blemish itself.
That's one of the most common frustrations I hear in consultation. Clients often tell me the active acne was annoying, but the mark it left behind feels more upsetting because it lingers, catches the light, and makes skin look uneven even when there are no fresh spots. The good news is that this usually isn't permanent scarring. It's often post inflammatory hyperpigmentation, and it can be managed with the right plan.
Table of Contents
- The Lingering Marks That Inflammation Leaves Behind
- What Is Post Inflammatory Hyperpigmentation
- Common Triggers and PIH Lookalikes
- Managing PIH with At-Home Skincare
- Advanced Professional PIH Treatments
- The Cornerstone of PIH Prevention and Management
- Your Treatment Journey FAQs and Aftercare
The Lingering Marks That Inflammation Leaves Behind
A very typical consultation goes like this. Someone points to their cheeks or jawline and says, “My acne is better, but the marks won't go.” Another client might mention eczema on the arms, a scratched insect bite on the leg, or a patch of irritation after waxing. The original problem settles, but the skin doesn't return to an even tone as quickly as expected.
That lingering mark is often what makes people feel their skin never looks fully healed. Makeup can cover some of it, but not always. Skincare might help a little, but progress feels slow and uncertain.
Practical rule: If the skin is flat but discoloured, you may be dealing with pigment rather than a textural scar.
Post inflammatory hyperpigmentation, often shortened to PIH, is the name we use for this type of mark. It happens after the skin has been inflamed or injured. Acne is a very common cause, but it isn't the only one. Eczema, bites, picking, friction, burns, and poorly managed aftercare after treatments can all play a part.
What confuses many people is that PIH doesn't always look dramatic at first. In some lights it seems faint. In others it appears much darker. It may also fade unevenly, which makes skin tone look patchy for longer than you'd like.
A calm, realistic approach matters here. Some marks respond well to home care and time. Others need clinic treatment because the pigment is sitting deeper or because ongoing triggers are keeping it active. The aim isn't to throw every product at your face. It's to work out what kind of pigmentation you have, what caused it, and what will move it on without irritating the skin further.
What Is Post Inflammatory Hyperpigmentation
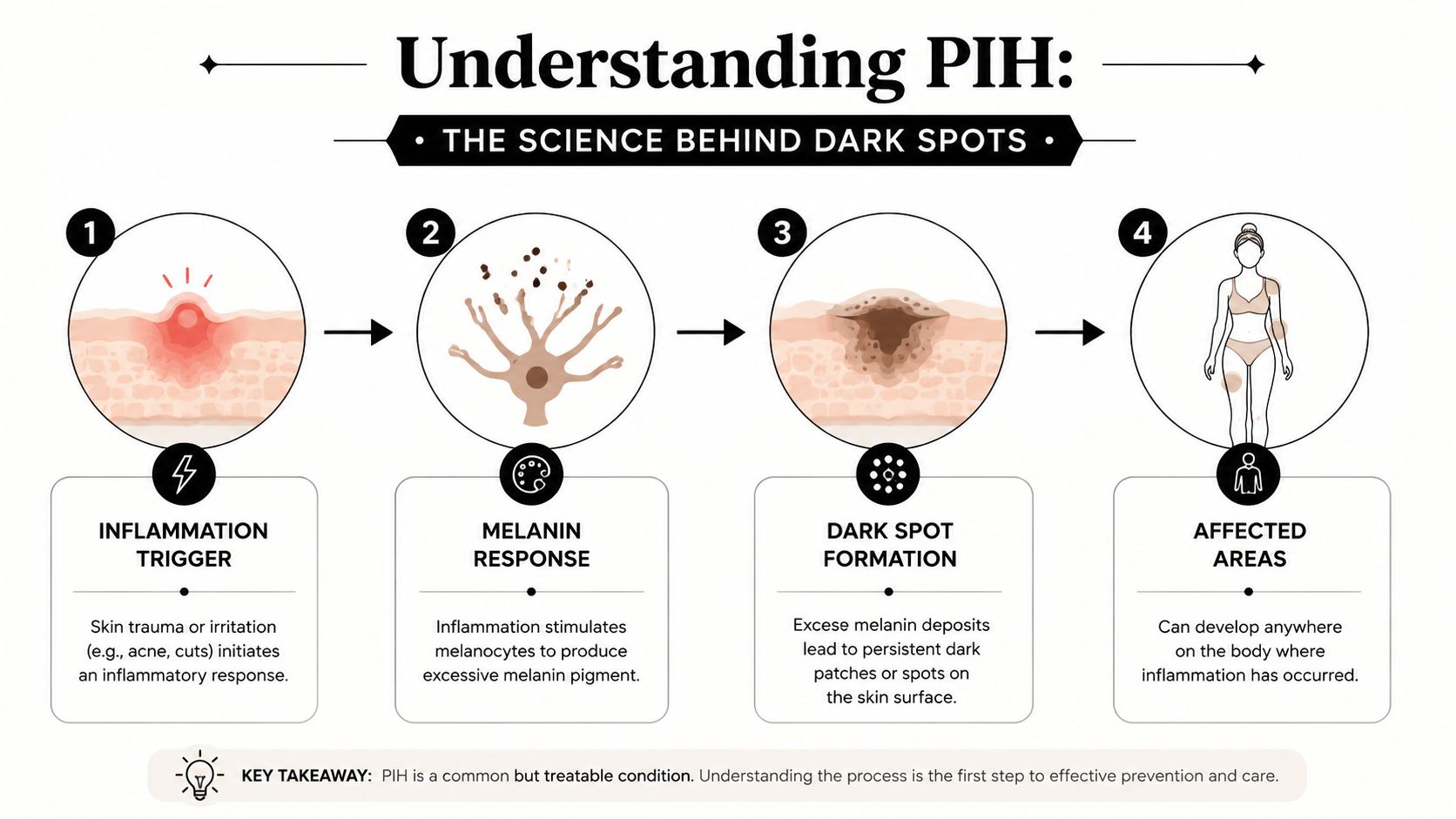
Post inflammatory hyperpigmentation is discolouration that appears after inflammation. The skin reacts to irritation by producing or distributing pigment unevenly, and that leaves a mark behind once the original spot, rash, or injury has healed.
A simple way to understand it
The easiest way to think about PIH is as an ink response. Your skin has pigment-producing cells called melanocytes. When inflammation happens, those cells can become overactive. Instead of returning quietly to normal once the irritation has settled, they can leave extra “ink” in the area.
That's why a pimple can disappear but a mark remains. The blemish has gone. The pigment response hasn't fully settled yet.
PIH is especially common in deeper skin tones. A review in the Journal of Clinical and Aesthetic Dermatology notes that over 65% of African Americans experience symptoms, and reports that 65.3% of African Americans, 52.7% of Hispanic individuals, and 47.4% of Asian individuals experienced PIH following acne inflammation; it also notes that epidermal PIH may persist for 6 to 12 months even with treatment in some cases (JCAD review of PIH in skin of colour).
If you want another plain-language overview of how brown marks form and why they differ from other pigmentation concerns, Dr. Chernoff on brown spots is a useful supporting read.
Surface pigment and deeper pigment
Not all PIH sits at the same depth, and that changes both appearance and treatment response.
| Type | How it often looks | What it usually means |
|---|---|---|
| Epidermal PIH | Brown or tan | Pigment is more superficial and usually easier to shift |
| Dermal PIH | Blue-grey or slate-toned | Pigment sits deeper and often needs more patience or professional treatment |
A flat brown mark after a breakout often suggests more superficial pigment. A greyer, more stubborn patch can point to deeper involvement. That's why two people with “dark marks” can need very different treatment plans.
A mark can be fading and still look noticeable. Slow improvement doesn't mean nothing is happening.
This is also where expectations need to be realistic. If the pigment is deep, pushing the skin too hard with harsh exfoliation often backfires. Calm, steady treatment usually works better than aggressive self-treatment.
Common Triggers and PIH Lookalikes
PIH doesn't appear out of nowhere. Something irritates or inflames the skin first, then pigment follows.
What commonly sets PIH off
Acne is one of the biggest triggers I see. A spot becomes inflamed, it's squeezed or picked, and once the swelling settles there's a mark left behind. The same can happen with cystic breakouts, shaving bumps, ingrown hairs, or irritation after hair removal.

Other common causes include:
- Eczema and dermatitis because repeated inflammation keeps the skin in a reactive state.
- Insect bites and scratching because trauma plus rubbing can deepen the pigment response.
- Heat, friction, and picking because physical irritation can prolong recovery.
- Poor aftercare after treatments if skin is exposed to too much sun or strong actives too soon.
- Sun exposure after inflammation because pigment cells are more easily triggered in healing skin.
If sun damage is part of the bigger picture as well, it helps to understand how it overlaps with uneven tone. This guide to sun damage skin treatment explains that broader context well.
Conditions people often confuse with PIH
Self-diagnosis often goes wrong because not every dark patch is PIH.
Melasma usually appears as broader, more symmetrical patches, often influenced by hormones and sun exposure. It commonly shows up on the forehead, cheeks, upper lip, or temples, and it doesn't always follow a single inflamed spot.
Sun spots or age spots tend to come from cumulative sun exposure rather than one clear injury or breakout. They often appear on areas that get repeated daylight exposure.
There's also another common post-breakout mark people mistake for PIH. Sometimes the leftover mark is more red or pink than brown. That points away from pigment and towards lingering vascular change. If the wrong treatment is used, progress can stall because the mark isn't pigment-led in the first place.
A few clues can help:
- PIH often follows a clear inflammatory event such as acne, eczema, or a scratch.
- PIH tends to be flat rather than raised.
- PIH is usually brown, tan, or grey-toned, not bright red.
- PIH often appears exactly where the inflammation was, rather than in a broad symmetrical pattern.
If a mark looks “similar” to something you saw online, that doesn't mean it's the same condition. Pigment disorders overlap visually all the time.
That's why a professional assessment matters. The right treatment starts with the right label.
Managing PIH with At-Home Skincare
Home care matters because PIH responds best when the skin is kept calm, protected, and consistent. Individuals often get into trouble when they try to treat marks by stripping the skin barrier.
The routine that usually makes the most sense
For at-home management, I usually want clients thinking in terms of roles, not trends. Each product should do a job.
A simple approach often includes:
- A gentle cleanser that removes oil, sunscreen, and makeup without leaving skin tight.
- Azelaic acid or kojic acid if pigment and inflammation are both part of the picture.
- A retinoid if the skin can tolerate it, because it supports cell turnover.
- A supportive antioxidant such as vitamin C in the morning if it suits your skin.
- A barrier-friendly moisturiser to reduce irritation from active products.
- Daily broad-spectrum sunscreen because no brightening routine holds up without it.
Retinoids are useful because they act a bit like a fast-forward button for how skin sheds and renews itself. Azelaic acid is helpful because it can support a calmer, more even-looking complexion while also fitting well into acne-prone routines. Kojic acid is another pigment-focused option that some people use well in carefully balanced formulas.
If you're curious about topical brightening ingredients and how they're commonly used to brighten dark spots, that overview is a sensible companion read.
A clinic may also recommend supportive treatments when inflammation is a major driver. For example, Dermalux LED therapy is often used alongside skincare because calmer skin generally responds better than irritated skin.
Why hydroquinone needs caution in the UK
Hydroquinone often comes up in conversations about pigmentation, and it's important to handle that topic responsibly. In the UK, hydroquinone 2% is unlicensed for PIH and banned in commercial skin lighteners, although specialists may initiate it under shared care in specific situations (Patient.info guidance on post-inflammatory hyperpigmentation).
That matters because people often buy unregulated products online hoping for a shortcut. With PIH, especially in darker skin types, that can go badly. The skin becomes irritated, barrier function suffers, and pigmentation can become more stubborn rather than less.
So the message isn't that every strong active is wrong. It's that unsupervised use of strong pigment agents is risky.
A safer home routine usually follows three principles:
- Start slowly so you can tell what your skin tolerates.
- Don't stack too many actives at once because irritation itself can prolong pigment.
- Keep the barrier healthy because inflamed skin doesn't brighten well.
The strongest home routine is usually the one you can stick to without triggering fresh inflammation.
Advanced Professional PIH Treatments
When PIH is deep, long-standing, or not responding well enough to home care, clinic treatment can make a meaningful difference. Professional treatments don't replace skincare. They enhance its effectiveness.

When home care reaches its limit
There are a few signs that suggest it's time to think beyond topical products:
- The marks are very persistent and barely shifting.
- The tone looks grey or blue-grey, which can suggest deeper pigment.
- You're improving the breakouts but not the aftermath.
- Every new spot leaves another long-lasting mark.
- Your skin gets irritated before it gets better with home exfoliation.
Effective treatment requires a specific approach. Different tools target different parts of the problem.
Chemical peels and microneedling
Chemical peels can help when pigment is more superficial and skin tone looks dull or uneven. The goal isn't to “burn off” pigment. It's to create controlled exfoliation so the skin renews more efficiently.
Peels can be useful for:
- post-acne marks that sit more on the surface
- uneven tone with congestion
- clients who want a structured course rather than random at-home experimentation
For anyone comparing how clinics explain these treatments, this page on chemical peels Southsea is a decent reference point for what a peel-based approach generally involves.
Microneedling, including 3D Dermaforce-style treatment, is a different route. It creates controlled micro-injury in the skin to encourage repair and improve overall texture and tone. This can be helpful when PIH overlaps with roughness, post-acne textural change, or a generally uneven skin surface.
The best treatment isn't the most aggressive one. It's the one your skin can recover from well.
Microneedling usually works best when active acne is reasonably controlled first. If fresh inflammation keeps happening, the skin is trying to heal in two directions at once.
Laser treatment and supportive LED therapy
For stubborn pigmentation, laser can be one of the most targeted options because it focuses on the pigment itself. Evidence reviewed in a 2024 paper found that with 1064 nm QS Nd:YAG laser treatment, 75% of patients achieved good improvement of 50 to 74% and 20% achieved excellent improvement of 75 to 100% (2024 review of PIH treatments).
That matters because it shows why clinic-based pigment treatment can outperform topicals alone when the pigment is more established.
At 3D Aesthetics Leamington Spa, one option for appropriate cases is 3D Nanosure pigmentation removal, which is designed to target pigmentation concerns with laser technology. In practical terms, this type of treatment is considered when marks are proving resistant, when precision matters, or when a client wants a treatment plan built around more than just creams and serums.
Supportive care around treatment matters too. Dermalux LED is often used as an adjunct because calmer skin tends to heal more comfortably and tolerate a course of advanced treatment better. It doesn't replace pigment-targeting treatment, but it can support recovery and help reduce the inflammatory environment that feeds the cycle.
A professional pathway often combines methods rather than relying on one. For example:
| Concern | Often considered |
|---|---|
| Superficial post-acne marks | Peel-led plan plus skincare |
| Pigment with texture changes | Microneedling plus brightening home care |
| More stubborn or deeper pigmentation | Laser-led approach with strict sun protection |
| Reactive or inflamed skin | Barrier support and LED alongside the main treatment |
That combination approach is often where people finally stop feeling stuck.
The Cornerstone of PIH Prevention and Management
If you do everything else right but skip sun protection, PIH usually lingers longer and can darken more easily. This is the part people underestimate most.
Why sunscreen changes everything

PIH and sunlight have a difficult relationship. Healing skin is vulnerable, and pigment cells are easier to trigger after inflammation. That means even if the original breakout or irritation is gone, daylight can keep feeding the mark.
In UK guidance, daily broad-spectrum sunscreen with SPF 30+ and protection against UV and visible light is described as the cornerstone of PIH management, with reapplication recommended at least three times daily to help prevent further darkening, as noted in the earlier JCAD review.
That can sound excessive until you realise what sunscreen is doing here. It isn't just “general skincare”. It is active protection for skin that is already trying not to overproduce pigment.
The habits that stop marks getting darker
The most useful prevention habits are usually simple:
- Wear broad-spectrum SPF every day even when it's cloudy.
- Reapply consistently if you're outdoors, near windows, or wearing makeup for long hours.
- Don't pick healing spots because extra trauma often means extra pigment.
- Treat acne and irritation early so the inflammatory cycle doesn't keep repeating.
- Follow aftercare properly after professional treatments because healing skin needs protection, not experimentation.
For a quick visual explanation of why this matters so much, this video is helpful:
Sun protection protects your results as much as it protects your skin.
That's especially true if you've invested in peels, microneedling, or laser. Without daily SPF, you make it far easier for old marks to stay visible and for new ones to form.
Your Treatment Journey FAQs and Aftercare
How long does it take to see improvement
This depends on the depth of pigment, the trigger, your skin tone, and how consistent you are. Surface-level marks can improve gradually with steady skincare and sun protection. Deeper pigment usually asks for more patience and often responds better when professional treatment is added.
One of the biggest mindset shifts is accepting that PIH doesn't vanish overnight. It clears by degrees. You may first notice that the edges soften, makeup sits better, or the mark no longer looks as dark in every light.
Can PIH come back after treatment
It can come back if the trigger returns. If acne continues, if you keep picking, or if sun exposure isn't controlled, new marks can form even after old ones improve.
That doesn't mean treatment failed. It means PIH management always includes prevention.
What aftercare matters most
After advanced treatment, aftercare usually centres on keeping the skin calm and protected.
Focus on:
- Gentle cleansing rather than scrubbing
- Good hydration with bland, barrier-supportive moisturisers
- Strict SPF use every day
- Avoiding picking, rubbing, or strong actives too soon
- Following the clinic's timeline for restarting exfoliants or retinoids
If laser has been used, you may also be advised to avoid heat, vigorous exercise, and unnecessary friction for a short period while the skin settles.
When should you stop trying to fix it yourself
A consultation is worth it when marks aren't shifting, when you're not sure whether you're dealing with PIH or something else, or when every new blemish leaves another dark patch.
It's also time to get help if:
- your skin is becoming irritated from multiple actives
- the pigmentation looks grey and stubborn
- acne and pigmentation are happening together
- you want a treatment pathway rather than more trial and error
The right plan usually feels calmer, not more chaotic. You should know what you're treating, why you're treating it, and what realistic progress looks like.
If you're dealing with post inflammatory hyperpigmentation and want a clear, personalised treatment plan, book a consultation with 3D Aesthetics Leamington Spa. A proper assessment can help you work out whether your marks are likely to respond to home care, whether you'd benefit from treatments such as peels, microneedling, LED, or laser, and how to protect your skin so the results last.